Book Appointment
Fillup the form to make an appointment with the doctor
Patient Information Understanding Knee arthritis
Arthritis is mostly wearing away of the smooth glistening cartilage which covers the ends of bone inside a joint and ensures smooth movement. When the cartilage is worn off, there are changes in the bone, which mainly hardens the bone (known as eburnation) and when bone rubs against bone leads to symptoms of arthritis.
OA is the most common form of arthritis where the surface cartilage is worn off and is a disease of old age. It is more common after 60 years and is rare in patients less than 40 years of age.
OA is known to affect certain joint regions of the body. It is most commonly seen in the Base of thumb, Knee, Spine, and fortunately is rare in the hip joints in the Indian subcontinent.


Pain in the joint is an essential feature of any arthritis. Swelling, stiffness, cracking sensation in the joint are all part of the arthritis picture. The fundamental association of OA is with activity. OA pain begins with activity, and it subsides when rested. “Crepitus” is a noise that is felt/heard. It is caused either when there is inflammation in the knee joint with thickening of the joint lining called synovium or when the surfaces are completely worn off and friction of the rough joint surfaces. Most symptoms of OA are associated with activities like climbing stairs, squatting, or sitting cross-legged on the floor and is partly relieved when these activities are modified. If arthritis involves the spine, that is called “spondylosis,” leading to stiffness, pain, and decreased the mobility of the back.
Certain general risk factors predispose an individual to OA. Old age, female sex, Race are some of the non-modifiable risk factors. Obesity is an important modifiable risk factor. Previous joint or cartilage damage is also a significant determinant in predisposing to OA knee. Any arthritis that develops without any predisposing factor is a primary OA, while if it has an association which predisposes, it is Secondary OA.
Some of the causes of secondary OA is trauma when the cartilage itself could be damaged. Crystal diseases like gout and CPPD crystal deposition cause inflammatory damage to the cartilage. When the nerves around the joints lose their sensitivity, it is neuropathic arthropathy ( commonly in Diabetics, syringomyelia) that can lead to secondary arthritis. Any young age malalignment of the hip, knee ankle axis can also predispose to a degenerative process and lead to arthritis.

Aging influences joint degeneration in a complicated way. The cartilage itself will sustain damage by repeated loading. Joint stabilizers like ligaments and muscles also lose their vitality, increasing the risk of damage to the cartilage.

The obesity epidemic is, unfortunately, sweeping the Indian subcontinent and has shown to increase the risk for many illnesses like Diabetes, Hypertension, Cardiac problems, and even cancers. Unfortunately, obese individuals are at risk of developing knee OA almost four times as their risk for developing hypertension. So, Obesity has a robust modifiable association with OA. Extreme Obesity (defined as Body Mass Index BMI- of more than 40) has more than tenfold increased risk to develop OA of the knee joints.

OA based on history, Physical examination, and X-rays. OA of the knee joint typically has a long-standing history of pain in the joints. Stiffness in OA lasts less than half an hour. Generally, arthritis is considered to have minimal inflammation so that markers like ESR are less than 40/hour, and importantly X-rays show cartilage damage and narrowing of the joints.
X rays are taken to demonstrate arthritic changes. In weight-bearing joints like the knees, it is useful to take X-rays in the standing position to determine the extent of the damage. Mostly 2-3 views are recommended to understand the real extent of cartilage damage.
The knee joint has three compartments. As shown in the image, the inner side is medial, the outer is lateral, and the joint space between the knee cap (patella) and the thigh bone (femur) is the patella-femoral compartment. With advanced degeneration of the knee joint, there is a complete loss of joint space and new bone formation, which is called as “Osteophytes.”
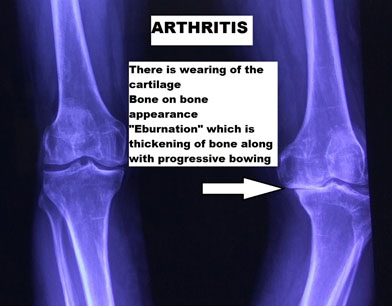
An interesting aspect of arthritic knee pain is, even though the cartilage itself is the primary structure that suffers the damage, the pain in OA is due to secondary changes that happen in the bone and surrounding structure. There is swelling (Bone edema) and thickening (eburnation), which develops in OA, which stimulates the pain-sensing nerves in the bone. The joints also have a sensitive lining called synovium, whose thickening and inflammation can also lead to knee joint pain.