Book Appointment
Fillup the form to make an appointment with the doctor
Total Knee Replacement Knee Preservation Surgeries
Knee preservation is a useful alternative for early arthritis. It is offered to patients who are not candidates for a joint replacement surgery with mild cartilaginous damage.
Patients who have single compartment changes in their 40’s are not ideal for joint replacement. Joint replacement in younger population will result in poor outcome and early failure. If a patient has a focal cartilaginous defect, that person also is not a candidate for joint replacement.
The available preservation techniques are-
It was considered to help with pain and improvement in the quality of life. Recently, evidence suggests that it is equivalent to placebo (sham surgery) and no longer recommended in the treatment of osteoarthritis. The only time it is helpful is-if there is a degenerated meniscus which has caused acute locking. Large scale reviews indicate that there is little to no role for standalone debridement for OA knee. http://www.cochrane.org/CD005118/MUSKEL_arthroscopic-debridement-for-osteoarthritis-of-the-knee
These are a group of techniques that are primarily done by arthroscopy in individuals who have limited cartilage damage. These techniques generally cannot be used in significant cartilage damage and are not to be done if there is all the three-compartment degeneration. Many sports injuries can be managed with these techniques and do improve the quality of life.
| Technique | Advantages | Disadvantages |
|---|---|---|
| Microfracture | Can be done with arthroscopic debridement
Not very expensive and easy surgical technique can be combined with high tibial osteotomy |
Regenerated cartilage of poor quality(fibrocartilage) |
| AMIC (Autologous matrix-induced chondrogenesis) | Single-stage surgery where a collagen patch is sewn onto a defect in the cartilage along with microfracture
Single-stage microfracture surgery and collagen membrane applied |
Has to remain non-weight bearing with limited knee bending for 4-6 weeks
Only helpful in a limited lesion of < 1.5cm cartilage defect |
| OATS Osteochondral Autograft Transfer/Mosaicplasty |
Helps in < 1cm sized defect
Single-stage surgery with cartilage taken from a healthy area as a plug and inserted into the defective area Restores Hyaline cartilage |
Donor site defect which will be non-weight bearing area and can have morbidity |
| ACI/MACI (Autologous Cartilage Implantation/Matrix assisted chondrocyte implantation) |
Hyaline cartilage itself is preserved | Two surgeries are required one to harvest the natural cartilage and a second one 3-4 weeks later to insert the cultured cartilage tissue into the defect.
Most expensive of the joint preservation procedures |
| OCA Osteochondral Allograft Taken from cadaveric donors |
Taken from cadaveric donors
Can be used for greater than 2 cm defect |
limited success rate of 20-40% Possibility of disease transmission Cost and lack of availability of donor makes it difficult in the Indian scenario |
The role of mesenchymal stem cells either from the same patient or from the placental tissue, has not been well defined. Previously, it had to be an open surgery to inject the stem cells into the joint; while with the present techniques, it can be done by injections. There is a lot of marketing involved with this technique with claims as a cure for arthritis, but at present, it is EXPERIMENTAL. Stem cell therapy has no long term proven benefit in arthritis management. Please consider the cost, risks, and benefit before subjecting oneself to experimental therapeutic interventions. In certain non-arthritis situations, stem cell injections have led to cancers, and one has to discuss the risks with the treating team very clearly.
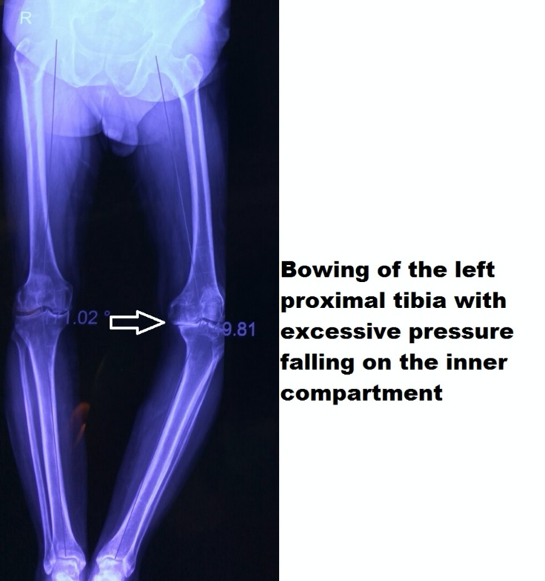
High tibial osteotomy is essentially an old technique where the joint is preserved by realigning the mechanical axis to acceptable alignment. The hip knee and ankle are essentially in the same straight line and in situations where there is deformity (bowing) of bone one side of the knee is worn out at a higher rate than the other side.
The most significant advantage of this technique is the ability of the individual to return to manual labor, usage of the squat toilet, and postponement of the need for joint replacement.
The idea of an HTO is to change the weight-bearing axis from the most loaded compartment to the lesser compartment with well-preserved cartilage. HTO as surgery will help to postpone the need for joint replacement in the 4-5th decade of life when the failure rates of joint replacement are much higher. The success rate of HTO is around 60-80% at ten years.
1. Flexion deformity in the knee (>150 )
2. Range of motion should be greater than 900
3. Ligament instability
4. More than one compartment arthritis ( patellofemoral arthritis, inflammatory arthritis like Rheumatoid arthritis)
HTO as a technique can be used for lateral compartment arthritis which is a rare entity less than 10% of the total patients who need HTO.
Two different HTO techniques as available. Medial opening wedge HTO (MOWHTO) and Lateral closing wedge HTO (LCWHTO) are used to slightly overcorrect the mechanical axis so that the weight-bearing axis goes through the lesser affected lateral compartment. The advantages and disadvantages of the techniques are mentioned in the table.
| Medial Opening Wedge HTO | Lateral Closing Wedge HTO |
|---|---|
| Easier to maintain the slope of the proximal tibia | Most commonly used technique |
| Needs a bone graft with a slightly expensive implant and needs non-weight bearing early six weeks | Early weight-bearing is possible |
| Lesser chance of compartment syndrome and damage to the peroneal nerve | No need for bone grafting and more straightforward implants can be used for fixation |
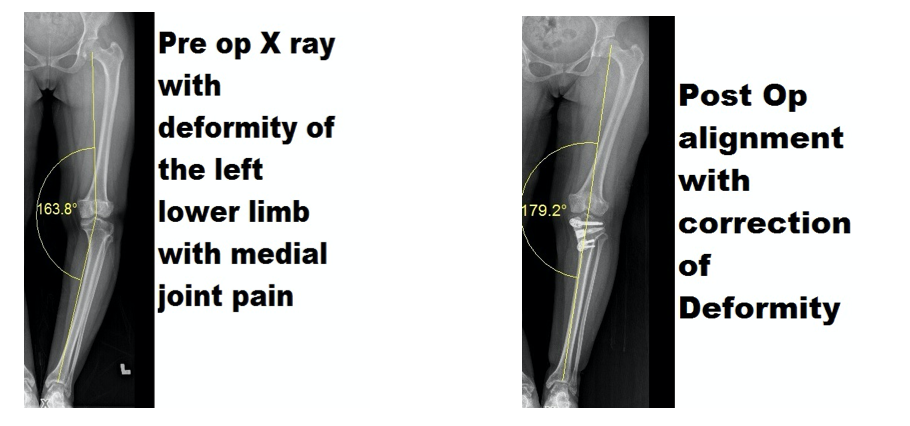
Medial opening wedge HTO is a technique that is used most often in sports medicine. In other non-arthritis deformities to correct the extremity alignment to prevent arthritis and in early OA to overcorrect the mechanical axis to improve the symptoms of arthritis.
A female patient with the congenital syndrome who had started to develop medial joint line pain with activity. Her symptoms prevented her professional career, and Medial Opening wedge osteotomy helped her functional recovery.
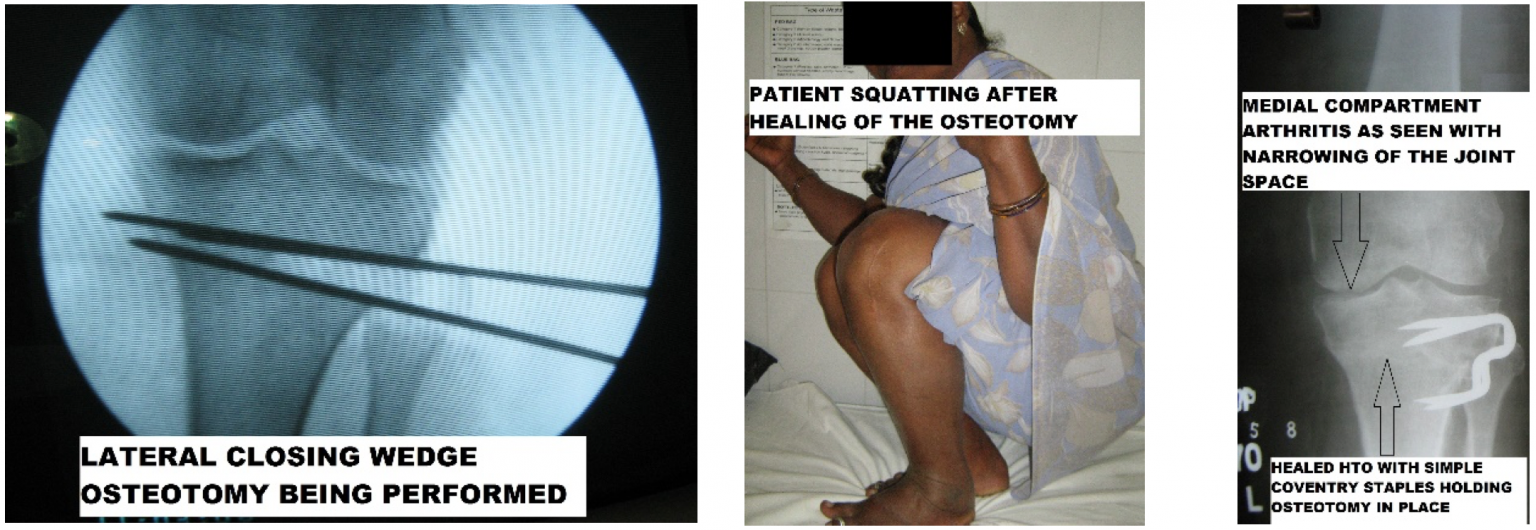
It is the earliest technique described and as shown in the table has some advantages over MOWHTO. LCWHTO is a simple technique that can be performed by most orthopedic surgeons with little equipment even in a smaller set up where there is an image intensifier available. The surgery itself does not require expensive implants, and patients will be able to walk with full weight in 3-4 weeks after surgery.
A 45-year-old female patient who is unable to perform her work as a garment laborer for six months and has been on leave of absence for her knee pain. She has no medical comorbidities and is from a poor socioeconomic background. At two years after surgery, the patient can perform most of her routine activities without the need for pain medication