Book Appointment
Fillup the form to make an appointment with the doctor
Health Professionals Intoeing its causes and management
A child walking with the toes pointing inwards is a common cause for concern in the pediatric age group. It is mainly due to a combination or individually of three clinical entities, Metatarsus Adductus, Internal Tibial Torsion & Increased femoral neck ante-version. Intoeing is one of the common concerns for which patients are referred to a pediatric orthopedic surgeon. It is mostly due to social pressure and comments; parents want the deformity assessed and usually pressurize the treating doctor for “some treatment.”
Metatarsus Adductus is a deformity where the big toe points towards the midline due to tightness in the Adductor Hallucis muscle. It has also been called “monkey toes” as it is seen in apes. This is a self-limiting disorder which needs only reassurance. Usually, rather than presenting as a deformity with only the big toe pointing inwards, it is part of more considerable deformity. The symptom complex is referred to as “Metatarsus adductovarus” which means that along with big toe pointing towards the midline, the sole also points inwards. This condition is commoner than the isolated “adductus” deformity. It is commonly noticed up to 24 months after which there is a tendency for automatic correction. Assessment of this deformity consists of pushing the ball of the big toe laterally to see if it crosses the midline and if it does not reach the midline or cross it, then we offer treatment for babies 3-6 months of age. The treatment will consist of serial casting, Adaptive shoes and braces till two years of age but usually individualized as per patient requirement

Internal Tibial Torsion is a deformity that is commonly seen in the age group of 6-24 months, and it usually resolves as the child grows older. This often presents as “in-toeing” and clumsy gait. Tibial torsion is primarily a clinical diagnosis. The best way to diagnose the tibial torsion is to look at a child in the seated position with the tibial tuberosity pointing forward then comparing the trans-malleolar axis (Line connecting the medial and lateral malleolus). A more straightforward method is looking at the 2nd toe and comparing the position of the tibial tuberosity with the 2nd toe position. Having the child lie prone on its abdomen and looking at the thigh and foot angle would also give an idea about internal tibial torsion. Usually, any associated deformity of the foot does influence the position of the 2nd toe in comparison with the trans-malleolar axis. Thus, we always recommend the trans-malleolar axis for the assessment of tibial torsion. The natural history of this disorder is such that it almost always resolves spontaneously, and very rarely does it need surgical correction. Various braces were used in the past; presently, there is no recommendation for bracing. Very infrequently would surgery be necessary; it consists of a de-rotation osteotomy of the distal tibia done in symptomatic kids.
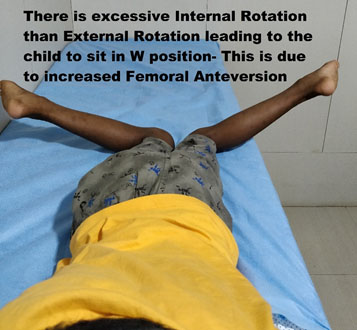
Femoral Anteversion is a condition where the intoeing is because of excessive forward pointing of the neck of the femur with respect to the knee joint line (the angle formed between the coronal plane and the neck of femur is called as ante-version. Most often, this condition presents in kids between 2-8 years of age and is equal in both the sexes. It manifests as excessive inward-pointing of the toes, especially when the child is tired, running. Parent’s complaint that the child sits in W position or reverse tailor position. The best way to examine this is to put the child prone and measure the amount of internal rotation (IR) and compare it to the opposite hip. Hip turned outside in the prone position is Internal rotation and turned inside is external rotation. In increased femoral anteversion, there is an excessive internal rotation of the hip, as shown in the picture.
Generally, there is a tendency for the hip joint to lose its range of motion as one ages and stabilizes by the time the child is in teen ages. Treatment of this condition is usually not warranted, and observation and reassurance are more than enough in its management.