Book Appointment
Fillup the form to make an appointment with the doctor
Conditions FLAT FOOT (PES PLANUS)
It is a situation where the medial arch of the foot is minimal or absent, leading to loss of the gentle curve of the feet and abutment of the inner end of the foot to the ground. Broadly, the flat foot is divided into flexible and rigid flat feet based on the symptoms and the way the hindfoot responds to stress.
There is about 13-15% incidence of flatfoot in adults. The exact percentage varies according to region and lifestyle. It is not the painless flat foot that one should be worried about but the painful flat feet that affect two distinct population. One in the teenagers where it could be because of the structural issue and another one in the elderly who could have a muscle dysfunction.
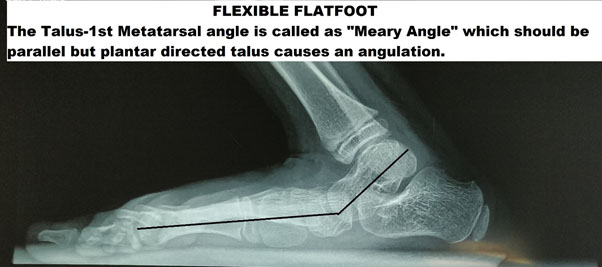
Flexible flat foot(FFF)- This is a condition where the arch is recreated when the individual stands on tiptoes but is absent when there is weight-bearing. FFF is mainly due to either ligamentous laxity or tight heel cord.
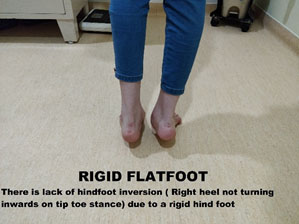
Rigid flat foot- This is a condition where there is limited hindfoot motion even when the individual is standing tiptoed. Either this is due to a bony problem, or there is a fusion of the bones of the foot called a tarsal coalition.

Congenital Vertical Talus (CVT- Rocker bottom Foot)
CVT is an entity where the foot arch is reversed with the convexity of the feet plantar wards. This appearance is the rocker bottom foot. It is due to the loss of the relationship of the bones of the mid-foot to the hindfoot.
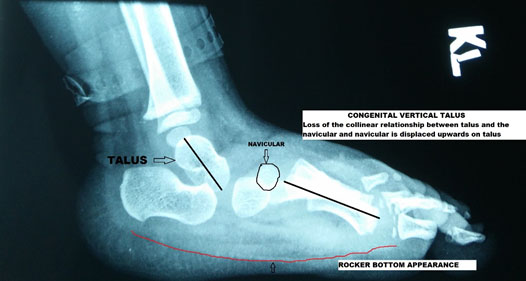
It is associated with genetic syndromes like myelomeningocele & arthrogryposis, and the functional outcome of the child is primarily determined by the associated anomalies. Symptoms include difficulty to walk and excessive heel contact, and the front of the foot has limited contact to the floor. X rays (as shown in the picture above) aid the diagnosis and can be helpful in planning treatment.
Previously, the procedure for this condition was an extensive surgery with soft tissue dissection, but presently the standard of care is to do a technique, which has been called “Reverse Ponseti Technique.” It consists of serial casting and limited surgical release for the soft tissue later on and with final open/closed reduction of the talonavicular joint and fixation with K wire.
In a salvage situation, we opt to perform a triple arthrodesis where calcaneus, talus, navicular, and cuboid are all fused to form a single bony mass. In some patients, we perform talectomy where the entire talus bone is removed so that calcaneus articulates with the tibia.
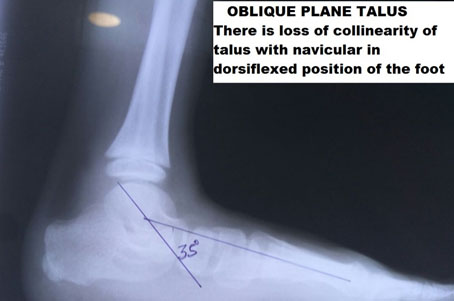
Oblique plane talus is an entity where the normal relationship of the talus and navicular is lost in dorsiflexion of the foot, but in plantar flexion, the relationship returns. This condition usually resolves with aging, but in certain situations, the child might need to undergo casting for quicker resolution of the problem.
A 3-year-old girl brought by parents with altered gait and occasional pain in the foot. Clinical examination and X-ray showed that the child had an oblique plane talus with pronated symptomatic gait. The child found it difficult to walk and thus was treated with a “Reverse Ponseti Method” of casting, and later on, a simple percutaneous naviculo-talar fixation was undertaken. Post-surgery the child has a planted feet stance and gait.

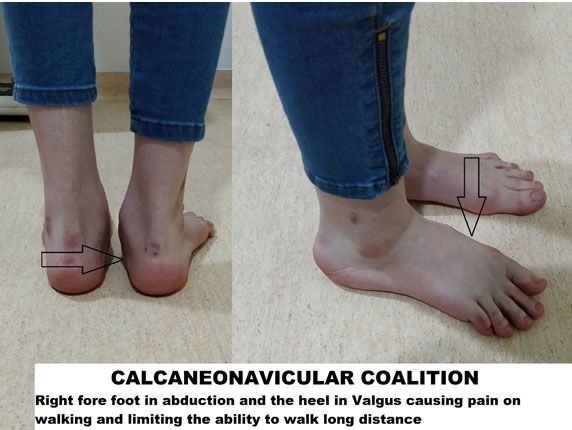
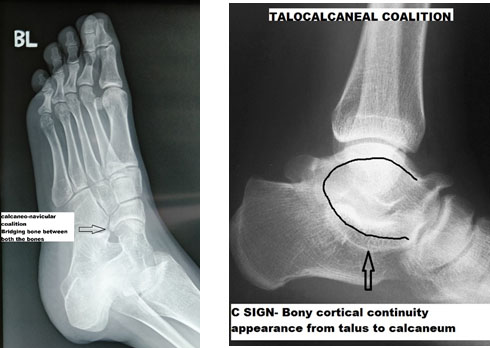
The coalition is an entity where there is an abnormal bony connection between bones of the hindfoot and midfoot, leading to lack of mobility in the hindfoot and thus flatfoot. Mostly it consists of two types of bony linkages called calcaneo-navicular fusion and the talocalcaneal fusion.
The calcaneo-navicular coalition is more common, and the kids are younger in the presentation (8-12 years) vs. Talocalcaneal coalition, which presents at a later age group of 12-15 years of age. The cause is primarily thought to be a failure of proper segmentation of the bone during in utero development. The coalition is noted in 1-2% of kids but is symptomatic in a far fewer number of them.
About 75% of the coalition are asymptomatic when they present; they present as recurrent ankle sprains, pain in the outer aspect of the ankle, or on the inner aspect — tiredness and fatigue of the feet after sporting activity.
On examination, the hindfoot is in valgus, and the forefoot is in abduction or nonprofessional terms; both the heel and the front part of the foot will be pointing outwards. Patients will have a decreased speed of gait. There is a limitation in the hindfoot motion in these patients and thus find it difficult to walk on uneven surfaces.
X-ray- The foot is imaged in three views. AP, weight-bearing lateral, and oblique view. In some patients esp. the calcaneonavicular coalition lateral view will show the bony bar.
CT/MRI- Advanced imaging modalities are recommended when surgical treatment is contemplated.
The first line of management of most of the coalition is conservative. The patient is immobilized with activity modification, and arch supports are selectively used. If no improvement is noted, then the treatment is escalated to surgical management
Excision of bony bar and interposition of soft tissue
This technique works well for calcaneonavicular coalition but is not very predictable for the talocalcaneal coalition. Fat or muscle interposition is done at the coalition site
If the patient has secondary degenerative changes that have developed or is not a candidate for excision of the bar, then the bones can be fused, and this is largely utilized for the talocalcaneal fusion with sub-talar fusion.

The accessory navicular is a common condition where there is an additional bone at the attachment of muscle called tibialis posterior noted in up to 12% of individuals. The junction between the accessory bone and the navicular bone has a fibrous attachment that inflames with repetitive trauma and leads to symptomatic flat foot in a small percentage of individuals.
Swelling can be present at the tibialis posterior insertion, limit the movement of the midfoot, and result in a flatfoot.
The treatment for Accessory navicular begins with conservative measures where physical therapy, activity, and footwear modifications along with Orthosis like the UCBL will give relief in a large number of patients. When none of these measures provide comfort, the patient can be subjected to surgery for excision and repair of the tibialis posterior tendon.
Flexible flat foot is a widespread clinical condition where the individual has an absent longitudinal arch but is symptomatic in only a small percentage of kids. New-borns are universally flatfooted, and the arch formation starts at the age of 2 years, and the maturity of the arch of the feet is at the age of 10 years.
This can be a reflection of certain familial tendencies, underlying neurological conditions like cerebral palsy, collagen disorders, or ligamentous laxity. The vast majority of children are idiopathic flat feet with no underlying problems.
The symptomatic flat foot child usually presents with pain and tiredness of the feet and difficulty to walk long distances because of pain in the feet. The patient will have hindfoot supination as shown before in the tiptoe test to differentiate flexible from rigid flat foot
Weight-bearing lateral/AP films will give as the idea of the relationship of the hindfoot to the forefoot. The talar axis should be parallel to the first metatarsal and is called the “Meary Angle.”