Book Appointment
Fillup the form to make an appointment with the doctor
Conditions DEFORMITIES
The entire specialty of “orthopedics” was born with the notion to correct deformity in children. It was coined by a French surgeon, Nicholas Andre, with its Greek origin, which means “Ortho,” “straight, correct,” and “paidos” is “child.” The specialty of orthopedics has expanded with the development of techniques of deformity correction, reconstructive surgery to improve the quality of life of patients.
The principles of deformity correction in pediatric orthopedics and even adults have continuously evolved, and there is a major contribution from various surgeons from across the world. The cross-pollination of ideas from the east by the techniques of Prof. Ilizarov and it’s adaptation with refinement from surgeons like Dr. Dror Paley has led to a rich heritage where the principles of deformity correction have been laid.
The deformity of the lower extremity are classified as-
The rotational abnormalities can be due to excessive femoral anteversion, internal tibial torsion. The angular deformities around the knee are called as Genu varus and Genu Valgum. The Linear abnormality is Limb Length Discrepancy, which is more common than recognized.
According to estimates based on military recruits, there is approximately 30% of healthy adults who have a 1-2 cm difference in the lower extremity length of both sides, which has no clinical significance.
The hip, knee, and ankle have to be in the same straight line or within three degrees ( as shown in picture 1) of alignment so that the weight is equally distributed and there is no long term effect. This is called the “mechanical axis,” and this alignment must be maintained after any surgical intervention. Most surgical intervention aims to recreate the mechanical axis alignment in the lower limbs so that there are no residual problems and hip knee ankle are in the same straight line.

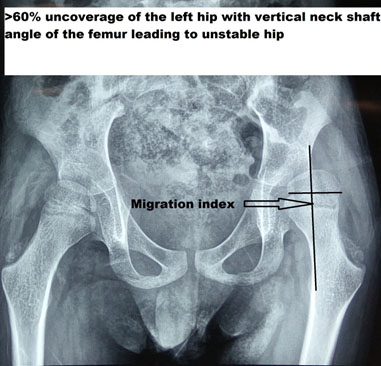
Various deformities are possible around the hip and can be femoral or acetabular. The femoral deformity is called “coxa Vara” when the head-neck angle is less than 120 degrees. If the same head-neck angle is more than 150 degrees, it is called coxa valga. Either of these problems is detrimental to the long term functioning of the hip and would need to be adequately addressed.
A CP child with “hip at risk’ and a high probability of dislocation of the left hip presented to us for evaluation. The patient was treated with Varus osteotomy and centering of the hip inside the socket piece ( acetabulum).
Knock knees
Knock knee is a deformity, also called as genu valgum. The knees touch each other, and there is a wide separation between the feet. This leads to unsightly gait and could be it could be part of a natural continuum, or it could be pathological. Most children end up being knock-kneed by the age of seven years, and it is part of the normal angular alignment evolution in children. But, if the genu valgus is more than 12 degrees after age seven or if the intermalleolar distance is greater than 8 cm, it is considered abnormal and needs to be investigated further.
A nonsurgical approach by bracing can be tried if the child is less than 6-7 years of age, and the angular deformity is less than 15 degrees. If there is a more considerable deformity, then the problem has to addressed surgically.

The surgeries for genu valgum are designed to correct the site of deformity, and the majority of times, the deformity is noted to be in the thigh bone (Femur). It can be treated either by an acute correction when there is little growth left or a gradual correction by “guided growth,” which means stapling the overgrown side ( medial or inner side) so that the outside of the knee catches up and the legs straighten out.
This patient had a previous knee surgery done with an angular deformity in both thigh and the leg bone, which was treated by a combined osteotomy so that an acute angular correction was obtained.
Genu varum is a deformity where there is bowing of legs and is a cause of significant anxiety to families. Most newborns have bow legs, and the deformity corrects by the age of 18 months. The newborn bow legs drift into neutral by 14-18 months and into more pronounced knock knees by the age of three years. It finally stabilizes to a subtle knock knee position by age seven years (3-5 degree valgus). There is a significant amount of anxiety in parents’ minds if the deformity is correctable, and presently there is a clear consensus that as long as the diagnosis is “physiological bowing,” there is a very high chance that the deformity will correct on its own.
Blount’s disease is a growth abnormality of the shin bone called tibia, where the upper growth plate shows pressure susceptibility and leads to the abnormality. There are two age groups when the deformity can develop either in a 2-5 year age group called infantile and >10 years called as adolescent blounts disease.
| Feature | Infantile Blount’s | Adolescent Blount’s |
|---|---|---|
| Clinical | 2-5 years, male-dominated, mostly both legs | >10 years, no sex predilection and mostly single leg |
| Risk factors | Early walking an obese child | Obesity |
| Treatment | Bracing and surgery | Surgery |
Example of an acute correction by distal femoral and proximal tibial osteotomy
Genu recurvatum – DEFORMITIES OF THE FEET
The foot acts like a tripod on which an individual can bear weight and walk. It has incredible suppleness and sturdiness to take the weight of the human body but still functions well. On weight-bearing, the foot acts like a spring to open out, and when an individual lifts the leg, it recoils back. There are some common deformities of the foot like a flat foot or pes planus and the high arched foot or the cavus foot.

Flexible flat foot is a condition when there is the absence of the medial longitudinal arch (the inner arch of the foot) on weight-bearing, but it is present when there is no weight put on the foot or when the big toe is lifted ( Windlass test). In an individual with a flexible flat foot, even though there is heel valgus when the person stands on tiptoes, the heel will swing into varus.
In comparison to the Flexible flat foot, the rigid flat foot is a deformity where there is no hindfoot motion and leads to pain and disability to walk. Common causes of the rigid flat foot are fusion problems in the foot called “Tarsal Coalition” or a “vertical talus.”
All newborns are flat-footed at birth; the arches of the feet start forming at two years of age and rapidly grow till around seven years of age. There is complete maturity of the arches by 12 years of age. In a Canadian army recruitment study, it was found that the incidence of the flat foot was about 15% of the hypermobile flat foot(Harris RI, Beath T. Army foot survey. Ottawa: National Research Council of Canada; 1947. pp. 1–268.). In an Indian study, it was found to be around 11.25%. (Bhoir et al. Prevalence of flat foot among 18 -25 years old physiotherapy students: a cross-sectional study. Indian Journal of Basic and Applied Medical Research; September 2014: Vol.-3, Issue- 4, P. 272-278). Most parents are concerned about flat feet in their newborns, and most often than not, the only thing they need is reassurance. Rarely newborn flat feet can have a problem like congenital vertical talus or even commonly oblique plane talus.
It usually presents as pain during activity and worsens with sporting activity. The treatment in the early stage is typically conservative with activity modification and footwear modification. When none of the traditional treatment works, surgical intervention is necessary.
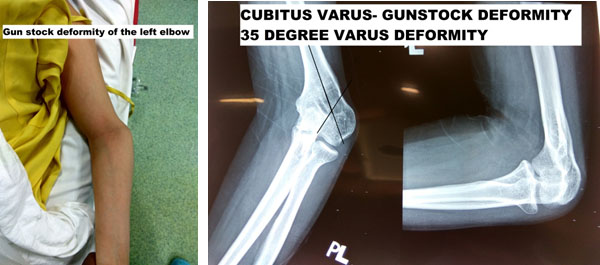
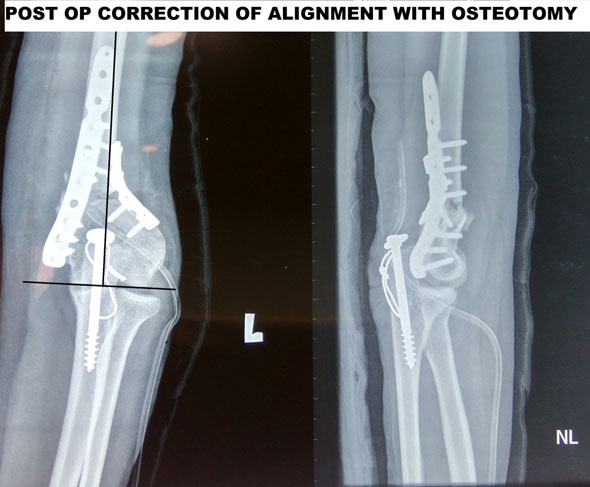
There are growth abnormality which occur in the upper limb which also can lead to significant problems of function. Some the common deformities are due to malunited elbow fractures. If a supracondylar humerus fracture has not healed properly it leads to a deformity called as cubitus varus and leads to a gunstock appearance. Many a times there is no functional deficit because of a supracondylar humerus fracture but will have cosmetic deformity.
Case Study-
Malunited Supracondylar humerus fracture in a 22 year old yemeni girl presenting for cosmetic appearance and also minimal weakness in the hand due to stretching of the Ulnar nerve.