Book Appointment
Fillup the form to make an appointment with the doctor
Total Knee Replacement Complex Primary TKR
The complex primary total knee arthroplasty represents a situation where the patient will present with problems that are of higher magnitude like a revision surgery but is getting the surgery done for the first time.
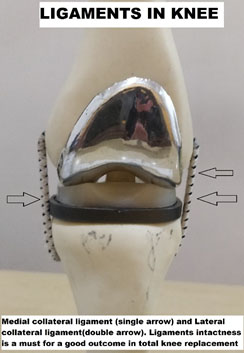
The knee joint has two ligaments on either side called as collateral ligaments whose intactness is necessary for a regular total knee replacement. If they were compromised, one would require more extensive surgery for a good outcome. Many times surgeons are not prepared to either handle ligament insufficiency or can happen as a surgical complication. The treatment would consist of implant design, which accounts for that insufficiency.
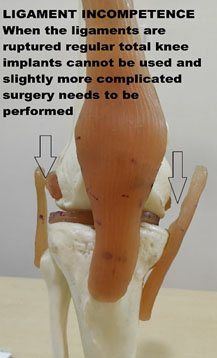
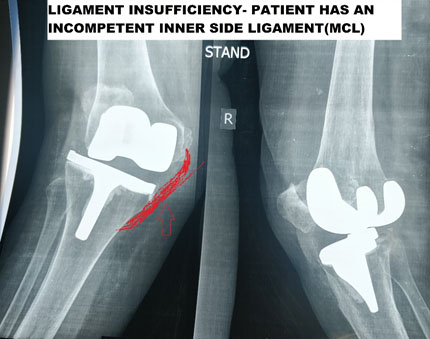
A 54-year-old male patient who had a ligament insufficiency underwent surgery with varus-valgus constrained prosthesis which protected the incompetent ligament.
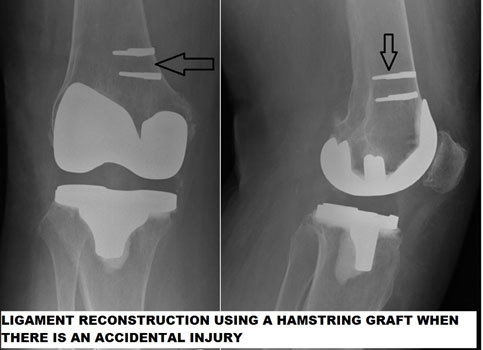
A 55-year-old female who had a knee replacement surgery during which a resident damaged the medial collateral ligament. The patient underwent a primary knee replacement with a reconstruction of the ligament with a hamstring graft, which was left distally attached, and repair undertaken on the inner side (medially) in the thighbone.

One of the pre-requisites for a knee replacement is the ability for the surgeon to be able to bend the knee to at least 90 degrees and perform total knee replacement. Unfortunately, there are certain conditions where the knee joint is stiff. The surgeon will have to use modified techniques to bend the knee during surgery for successful completion of total knee replacement.
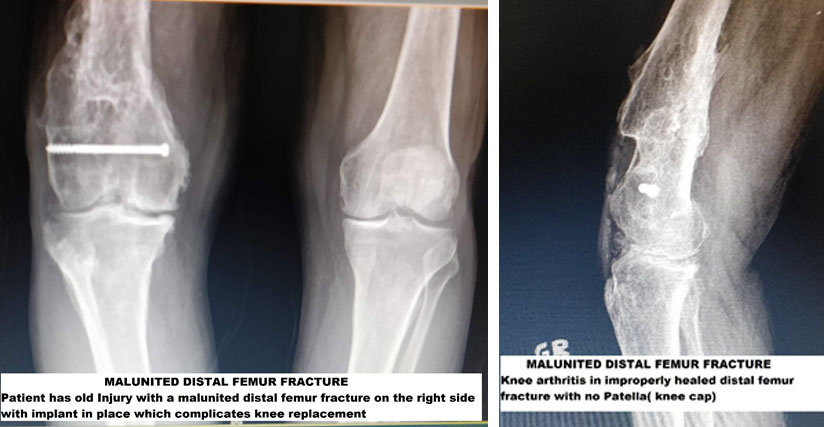
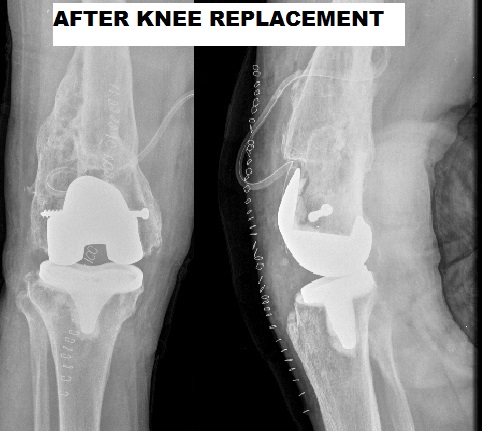
A 60-year-old Iraqi war victim has a history of multiple surgeries on his knee presents with deformity, pain, and inability to bend the knee. He was advised knee fusion, but the patient desires knee movement and some help in performing his activity of daily living. The patient underwent a total knee replacement with technical modifications so that his missing knee cap, adhered muscle and loss of axis in the thigh because of poorly healed thigh bone fracture was all taken into account.
This person had all the problems that are incumbent in a complicated knee replacement. His knee was stiff, no kneecap, and multiple scars in front of the knee. We undertook a knee replacement where we sequentially established the joint line, gained knee bending, created bony surfaces on which we could place the knee replacement prosthesis.
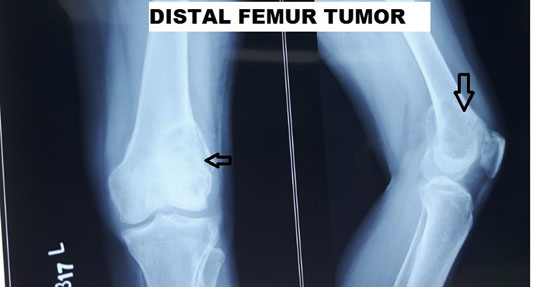
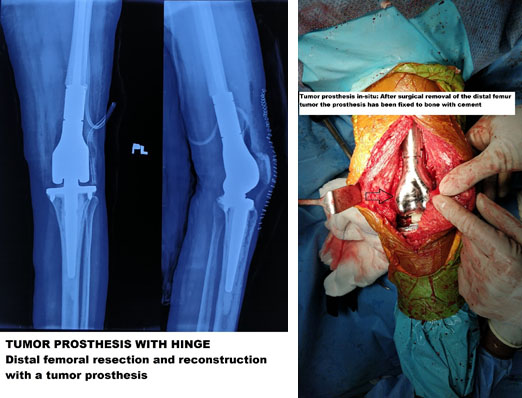
A 56-year-old woman presented with a biopsy-proven distal femur giant cell tumor. Patient’s lesion was not amenable to preserving the distal femur and thus excision of the entire distal femur and reconstruction with hinged knee prosthesis as a primary modality undertaken.