Book Appointment
Fillup the form to make an appointment with the doctor
Health Professionals Club Foot
Clubfoot is a complex foot deformity present at birth, which leads to a significant functional deficit if untreated and a source of anxiety to parents. Fortunately, the deformity can be treated, and the child can lead a healthy life without residual defects.
There is no definitive cause seen, but it is a genetically determined (about 25% incidence if a parent has a clubfoot). It is a fairly common childhood deformity with a reported incidence of 1 in 1000 in Indian population as well.
It can be associated with various syndromes like
Arthrogryposis
Tibial hemimelia
Myelodysplasia
The syndromic clubfoot is generally rigid and requires a more extended treatment for the betterment of the child.
C – Cavus ( tightness of the intrinsic muscles)
A – Adductus
V – Varus
E – Equinus
It is an easily identifiable entity, and the toes and sole of the feet point inwards. There is a collective entity called “positional” clubfoot, which primarily differs from the “structural” club foot, where the club feet are not correctable by passive forces. The positional clubfoot is mainly a packaging disorder where the foot can be passively corrected and is more due to external compression inside a tight uterus without a structural problem in the feet themselves. While in the structural club foot, there is a tight tissue tether that needs to be stretched out by constant pressure and the deformity correction obtained. Most often than not, the fully corrected foot is still going to be a little smaller than the regular foot, and it stays like that till skeletal maturity.

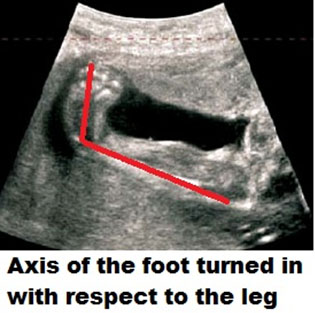
Presently, many clubfeet are recognized in utero during prenatal Ultrasound screening. It is an eminently treatable problem, and there is no need for anxiety for parents and individuals in its management.
The primary method of treating clubfoot is by a technique called the “PONSETI” technique.
Dr. Ponseti has revolutionized the treatment of clubfoot and has been a genuinely revolutionary intervention. Before the advent of the ponseti method, many patients ended up with a painful, stiff foot in order to correct a deformity. But, with the use of this elegant method, we can obtain excellent correction with little recurrence. In an advanced country like the USA, he published his experience in 1963 in a reputed journal called “Journal of Bone and Joint Surgery.” Unfortunately, most Orthopedic surgeons did not accept his method till the late ’90s until parent groups got active on the internet and sought his expertise was in demand and now is the standard of care across the world.

The serial POP casting of the feet weekly for 6-9 casts will help to obtain correction to most of the deformity except the equinus. In 80-90% of cases, the child needs a heel cord tenotomy to correct the deformity. We undertake the tenotomy in the operating room as there is complete control, and the child is relaxed. Many club foot kids do not have a dorsalis pedis artery. If there is an inadvertent injury to the posterior tibial artery during tenotomy, it can lead to significant problems of blood flow to the foot. Operating in the clinic has been advocated by Dr. Ponseti and has been done safely in large practices.

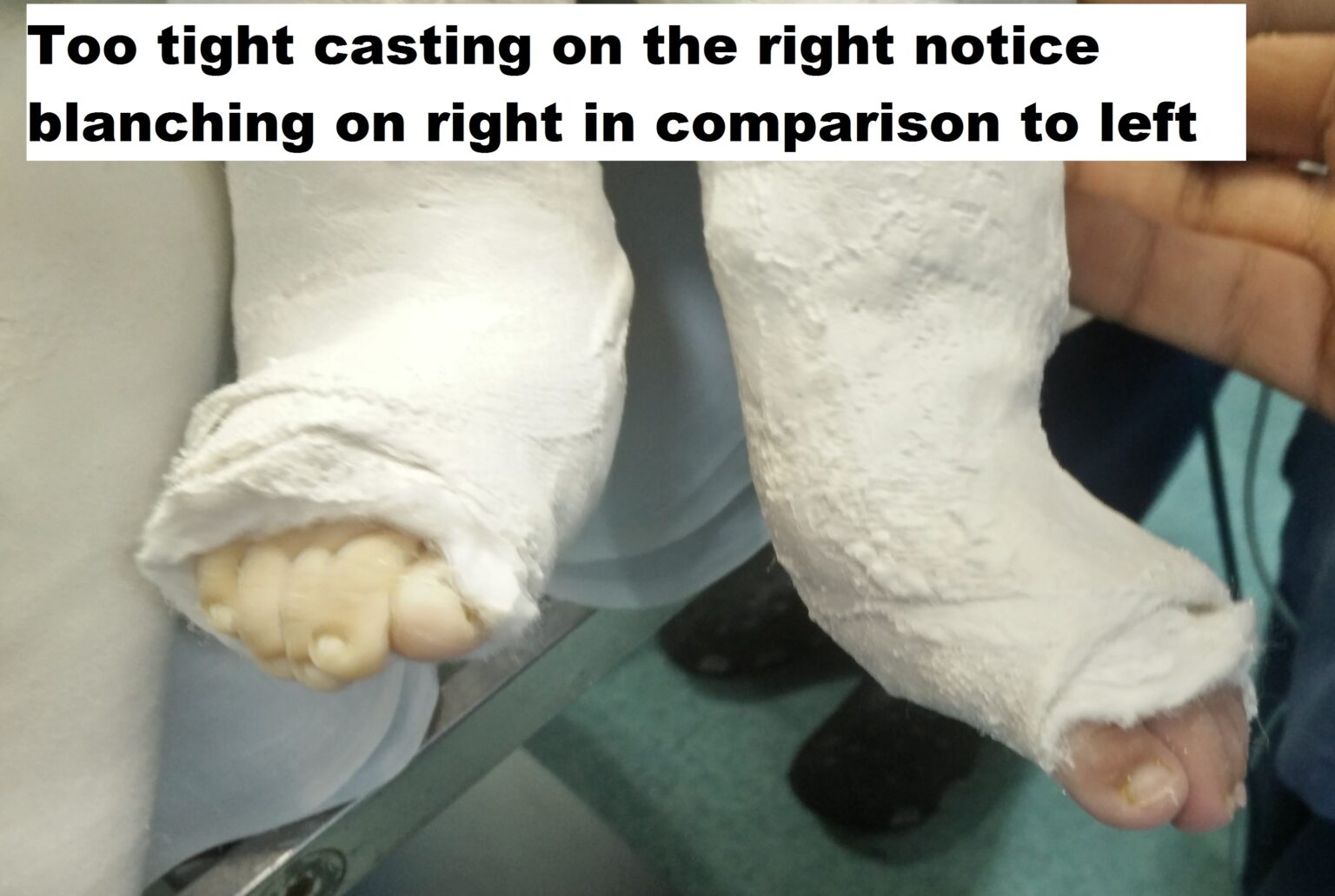
Post-tenotomy cast – 3 weeks
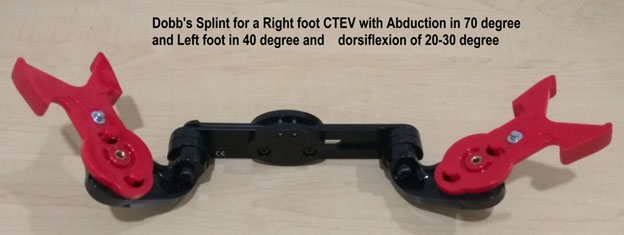
Bracing with Foot Abduction Orthosis- 22-23 hours for three months and later night time bracing for 3-4 years Dennis brown Splint/ Dobb’s splint are orthosis that helps maintain the correction of the deformity. The splints keep the affected foot in a 60-70 degree of external rotation and 20-30 degrees of dorsiflexion. The primary difference between the DB splint and the Dobb’s is the ability to move the feet independently in Dobb’s splint while both feet move together in Dennis Brown splint.
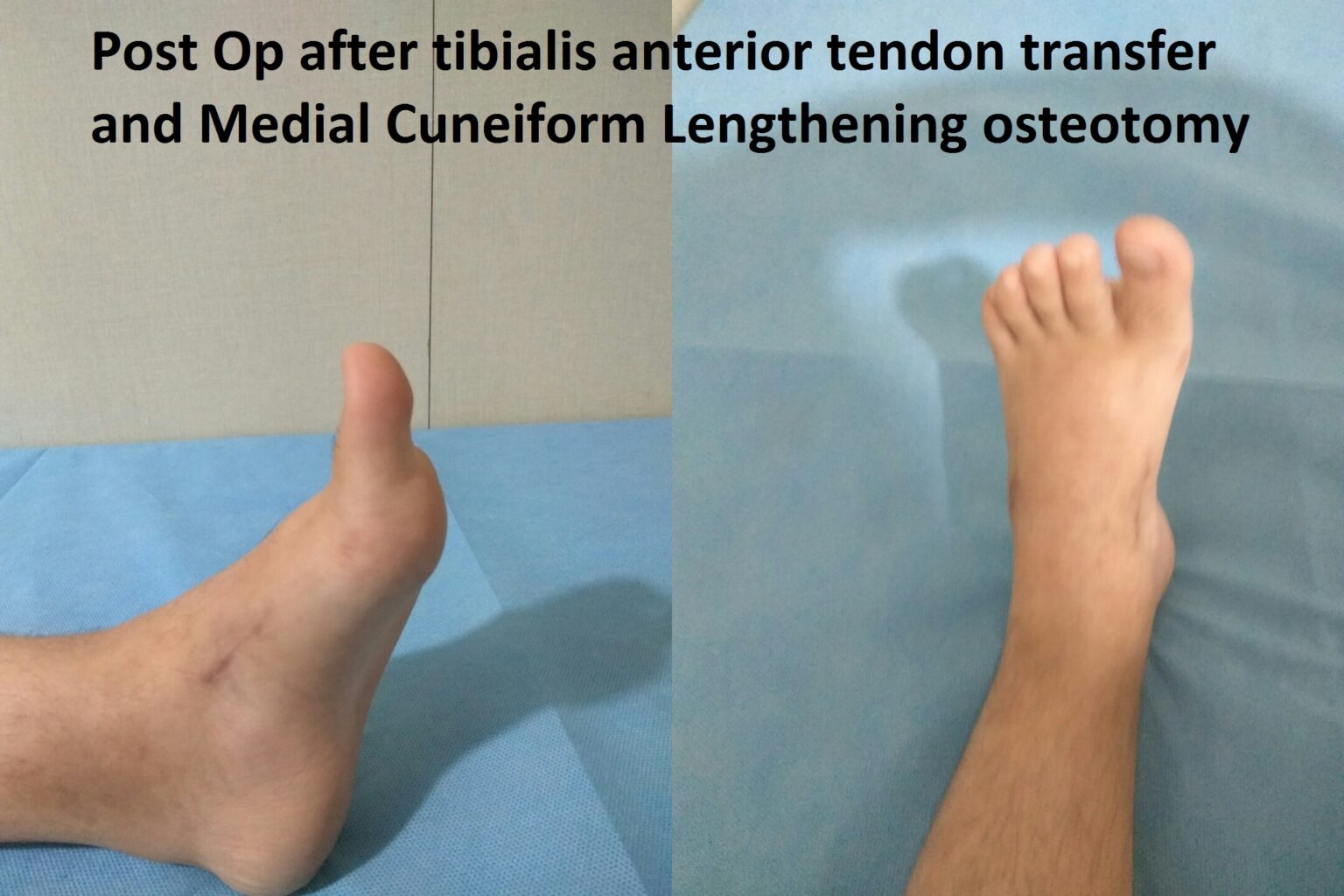
The recurrence is an unlikely phenomenon if a proper bracing protocol is followed. There could be minor relapse with dynamic supination and in-toeing when in 10-20% of patients, a Tibialis Anterior muscle transfer might be necessary.
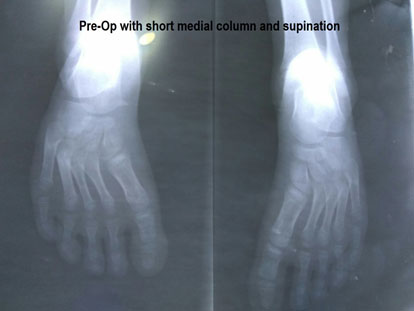
A 6-year-old girl presents with a recurrence of club foot. She developed dynamic supination and was treated with tendon transfer and medial column lengthening to get a good plantigrade foot.
Fortunately, the incidence of neglected club foot has been reducing. The lifelong morbidity of this condition can be disabling, and the treatment for neglected club foot can be major surgeries with stiffness almost always as a complication.

One of the most challenging things as a family for parents to accept is that their child has a congenital deformity. Isolated club foot is eminently treatable, and parents should not even remotely consider the option of abortion. The ethical and moral dilemma would be when the child has a complex congenital disorder, and club foot is part of the spectrum of abnormalities, and in those situations in concurrence with a geneticist, physician and surgeon families could make their informed choices.
It is advisable that ponseti casting is started within 7-10 days of birth to ensure good outcomes. The reason is that the foot is flexible at birth and gets rigid with the progression of time. The recommendation to postpone for a week is to let the skin mature a bit to avoid skin issues immediately after birth. Having said that- Ponseti treatment is effective even 2-3 years and in neglected deformity of the feet.
Ponseti casting is done on a 5-7 day interval for 5-8 cast changes during which the parents should note progressive changes in the deformity.
POP is a better material for the correction of deformity and is inexpensive. The soft cast material is also good enough to hold the correction but is generally quite expensive than a regular Plaster of Paris.
The maintenance of the correction is equally crucial after ponseti casting. DB splints or other corrective shoes do it. Parents need to understand that if the shoes are not used appropriately and for at least 3-4 years of life, the deformity can recur. Once corrected, there is no effect on the gait of the child, and in fact, clubfoot does not in any way delay the ability of a child to walk. You can still notice quite some club foot individuals walking with the deformity.
Parental anxiety leads to questions that are often perceived as unreasonable by health care delivery personnel. One of the issues that are often posed in the Indian scenario, is it possible to correct100%of the deformity and a guarantee to it? Our answer to such questions is that Ponseti is the most elegant and predictable method developed to date in the management of club foot. It gives the best results, and the correction is up to 95% of the babies in the nonsyndromic situation. The other point to remember is the compliance of families to wear the brace for the prescribed length of time
Well trained ponseti technicians can obtain a good result in club foot correction. But, one has to remember that if not correctly done, it could worsen the situation. To emphasize, the older method was called the Kite method, where the fulcrum was at the calcaneocuboid joint, which is about 1.5 -2cm behind the point where the ponseti way applies the corrective forces. That simple difference could make a massive difference in good and bad outcomes. If the heel cord tightness is corrected earlier before the supination, the child could develop a rocker bottom foot. The patient must understand that their surgeon is competent to do the job and inspire the confidence necessary to undertake this correction.
There is a 10-15% chance that the child might require a tibialis anterior tendon transfer after ponseti casting correction of the deformity. This is necessary to balance the foot with muscle forces, and the need for surgery is not treatment failure. Still, it is the continuation of the management of this complex deformity.
Club foot correction is a very visual phenomenon, and most parents can intuitively see the correction at each visit. For objective assessment, there are scoring methods like the Pirani scoring, where each component of the deformity is scored on a scale, and the correction can be objectified.