Book Appointment
Fillup the form to make an appointment with the doctor
Conditions Bow Legs
Genu Varus is a deformity where there is bowing of legs and is a cause of significant anxiety to families. Most newborns have bow legs, and the deformity corrects by the age of 18 months. The newborn bow legs drift into neutral by 14-18 months and into more pronounced knock knees by the age of 3 years. It finally stabilizes to a subtle knock knee position by age seven years (3-5 degree valgus). There is a significant amount of anxiety in parents’ minds if the deformity is correctable, and presently there is a clear consensus that as long as the diagnosis is “physiological bowing,” there is a very high chance that the deformity will correct on its own.
Blount’s disease is a growth abnormality of the shin bone called tibia, where the upper growth plate shows pressure susceptibility and leads to abnormality. There are two age groups when the deformity can develop either in a 2-5 year age group called infantile and >10 years called as adolescent blounts disease.
| Feature | Infantile Blount’s | Adolescent Blount’s |
|---|---|---|
| Clinical | 2-5 years, male-dominated, mostly both legs | >10 years, no sex predilection and mostly single leg |
| Risk factors | Early walking obese child | Obesity |
| Treatment | Bracing and surgery | Surgery |
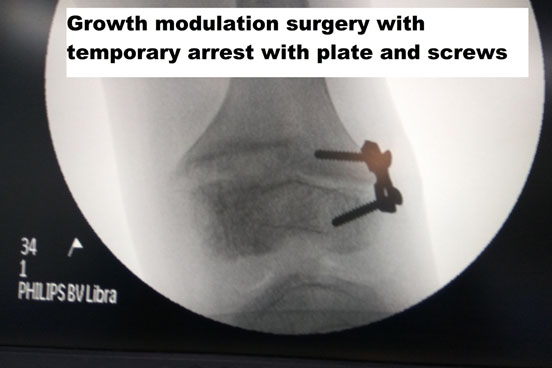
A 2 ½-year-old female obese child presented with features suggestive of Blount’s disease she had failed conservative treatment with bracing and needed surgery to correct her abnormality.



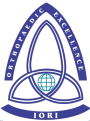
The age-related varus is primarily due to constitutional changes that happen in the bone, while the Blount’s bow leg leads to a growth disturbance and damage to the inner growth plate of the upper tibia. We measure the MD Angle, where an MD angle less than 10-degrees points towards a physiological bowing while > 16-degrees points towards a Blount’s bowing.
If a child has a mild abnormality, can wait till 18-24 months, if there is asymmetry, or if both the legs are pronounced in an overweight child, then it is better to consult a Pediatric Orthopedic Surgeon or at least the pediatrician for clinical examination.
If the child is overweight, who is an early walker, then excessive pressure is applied to the inner aspect of the growth plate over some time leads to growth arrest and its attending problem. It is mechanical overloading in a susceptible biological individual that leads to Blount’s disease.
There are conditions like hypophosphatemic rickets and metaphyseal chondrodysplasia, which can also lead to bow legs. Essentially the individual has short stature and has a widening of the growth plate at various locations. These patients usually need surgical management after appropriate medical management.
Inappropriate management of hypophosphatemic rickets leading to gross deformity in adulthood, stresses the need for proper counseling and surgical management for good clinical outcome. A 28-year-old female patient who had stapling done at a young age for rickets presents with gross abnormality and inability to walk. This case illustrates the need for periodic follow-up.
Physiological bowing-
Most children with physiological bowing do not need any intervention except periodic follow up. It is wise to see the doctor once in 6 months, and X rays are to be done if it persists more than 18 months of age
Blount’s disease
Early Blount’s with grade I &II stage up to the age of three years can be treated by bracing. If the child is obese or if there is a failure of bracing, then the child will require surgical treatment, please consult your doctor for the appropriate surgery.

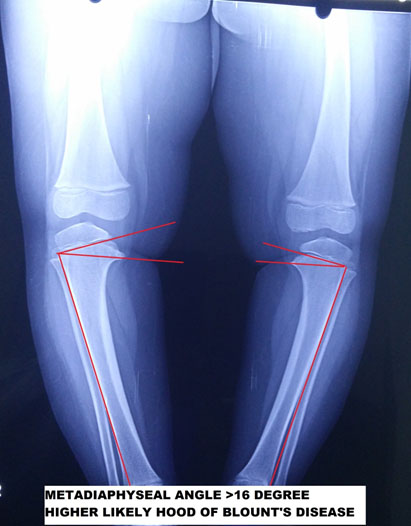
If there is adequate growth left ( age between 10-12 years), then the deformity can be treated with a simple surgery where the growth plates are temporarily held without growth by using plates that prevent bone from growing, and thereby deformity can be corrected.
If adequate time is not available for a growth modulation surgery (typically girls stop growing at 14 and boys at 16 years), then we will have to perform an operation called Osteotomy where the bone is broken. The deformity is corrected acutely, and proper mechanical alignment obtained.
A 17-year-old Iraqi girl with a metabolic abnormality presents with deformity and pain in the knee. She has gross varus and the difficulty to walk.
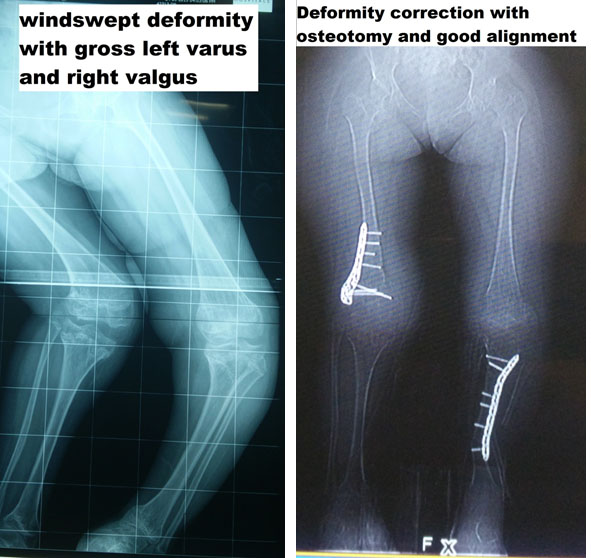
A girl with a complex congenital growth plate abnormality with windswept deformity (essentially one leg of bowing and the other knock knees) was treated with Osteotomy and deformity correction with good clinical outcome
Elderly patients do present with bow legs due to osteoarthritis changes in the joint and significant deformity with functional deficits when no other treatment is possible; then a joint replacement surgery is offered for correction of deformity as well as treatment for arthritis.
